
Out of Network vs. In Network: What the Research Actually Shows
- Accretive Health Advisors

- May 20
- 5 min read
This is the question I get more than almost any other, and for years the honest answer was a shrug and a story. Out of network feels like the bigger check because nobody is capping what you can bill. In network feels safer but smaller. Everyone has an anecdote and almost nobody has the data.
We finally do.
Two serious pieces of research, one in JAMA Health Forum and one in Health Affairs, let us stop arguing from feel and start arguing from numbers. Read them side by side and the picture is not the one most groups carry around in their heads.
Medicare Is the Ruler Nobody Talks About
Start with the measuring stick, because every honest version of this conversation runs through it.
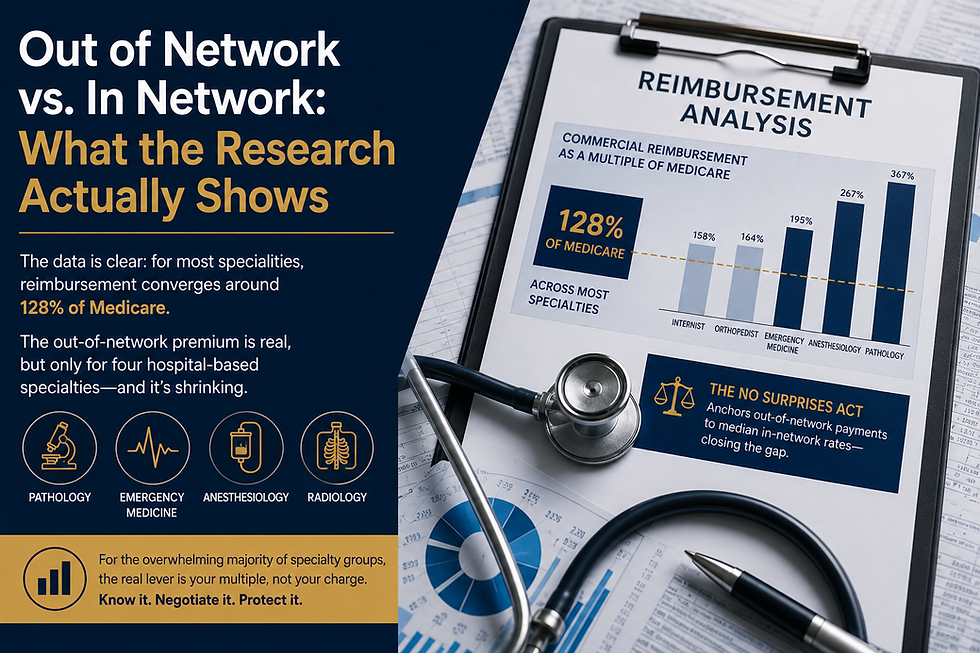
The JAMA Health Forum study, Duffy and colleagues in 2022, says it plainly. Across the commercial market, mean contracted rates for most physician specialties land at roughly 128 percent of Medicare. That is the water level the whole market floats on.
Your fee schedule is not really a number, it is a multiple of Medicare, whether or not anyone in your office ever says so out loud. If you do not know your multiple, you do not know your business. You just know your deposits.
The Out of Network Premium Is Real, But It Lives in Four Rooms
Here is where the myth is born. The premium people chase is real, but it does not live in the building most groups think it does.
The Health Affairs work, Cooper, Nguyen, Shekita, and Scott Morton in 2020, isolates four specialties: pathology, emergency medicine, anesthesiology, and radiology. These are the ones where the patient never picks the doctor. Nobody shops for the anesthesiologist the way they shop for an orthopedist. That single fact is the whole game.
Because the patient cannot walk around them, those physicians can stay out of network without losing a single visit, which hands them leverage no ordinary practice has.
The numbers show exactly what that doorway is worth. In that data, out of network charges ran from roughly four and a half to eight times the Medicare rate, with anesthesiology charges around 802 percent of Medicare and emergency medicine near 781 percent.
The leverage even bleeds into their in network deals. Where an internist sat at about 158 percent of Medicare and an orthopedist at 164 percent, those same four specialties were negotiating in network rates between roughly 195 and 367 percent.
That gap is not clinical skill. It is a locked door, and the toll for being allowed through it.
For Everyone Else, It Is a Mirage
Now lay the two studies on top of each other and the trap comes into focus.
The JAMA Health Forum analysis of more than seven and a half million emergency claims found in network payments running about 14 percent above the No Surprises Act benchmark, while out of network payments ran about 112 percent above it.
At a glance that reads like a green light to go out of network. It is not, and the reason is the first study. That 112 percent shows up in emergency medicine precisely because emergency medicine owns the locked door. Take away the door and the premium goes with it.
A dermatology group, a cardiology group, a primary care platform, none of them can hold a patient hostage in a hallway. So going out of network does not buy them leverage. It buys them a longer wait to get paid, a bigger pile of bad debt, and a patient holding a bill they never saw coming.
It was an oasis that was only ever real for four specialties standing in a corridor. Everyone else is walking hard toward water that is not there.
The funding split makes the same point from another direction. The premium was far larger in self funded plans, around 120 percent above the benchmark, than in fully insured plans at about 43 percent. The advantage was never evenly available. It always came down to who could not be avoided and which plan was holding the checkbook.
The No Surprises Act Quietly Moved the Anchor
Even for the four specialties that had the leverage, the ground is moving under their feet.
The No Surprises Act ties the out of network reference point to the qualifying payment amount, which is essentially the insurer's own median in network contracted rate for that service in that region, trended forward for inflation.
The arbiters who settle disputes are not permitted to look at the physician's billed charges, or at Medicare, or at Medicaid. The law took the one number that ever made out of network rich, the unbounded charge, and quietly walked it out of the room.
What is left on the table is a median in network rate that sits barely above the in network number to begin with.
We already have a preview of how that story ends.
When New York installed a similar arbitration system, the Health Affairs authors found it cut out of network billing by about 6.8 percent and pulled in network emergency physician pay down by about 9 percent.
The leash does not only shorten the out of network reach. It drags the in network rate down along with it.
Those same researchers estimated that if these four specialties were simply paid like orthopedists, the system would spend roughly 60 billion dollars a year less. That figure is the size of the prize, and the entire policy current is running toward giving it back.
The Real Lever Is Your Multiple, Not Your Charge
So strip it all the way down.
For the overwhelming majority of specialty groups and platforms, out of network is not a strategy. It is a story we tell ourselves about money that was never sitting there.
The real lever is unglamorous and far more durable. Know exactly where your in network rates sit against Medicare and against the live market, find the contracts that quietly drifted below that line, and negotiate the multiple up with the evidence in your hand.
That is the difference the data actually rewards.
Chasing a bigger charge is chasing a mirage. Raising your multiple raises the floor under every visit you will ever bill.
Where Accretive Health Advisors Comes In
This is the work we do.
At Accretive Health Advisors we benchmark reimbursement at the CPT level against Medicare and against market data drawn from hundreds of millions of posted rates, so a specialty group can finally see its real multiple instead of guessing at it.
We find the contracts running quietly below market, build payer negotiation strategies that move the in network rate in a direction you can defend in the room, and then make sure those gains survive the trip through the revenue cycle and land as actual cash.
No volume risk, no out of network mirage, just the one number that truly drives the business moved in the right direction.
More on how we think about this lives across the Accretive Health Advisors Blog.
If you run a specialty group or a multisite platform and you have ever wondered whether out of network would pay you more, the honest answer from the research is almost certainly no, not unless your patients cannot choose you.
The money you are hunting for is hiding in the contracts you already hold, priced as a multiple of Medicare you have probably never measured.
We built our practice to measure it and to close the gap it uncovers, and we work on a model where we only win when you do.
The smart move is to find out where you stand before the next contract cycle decides it for you.



Comments